When it comes to treating sexual dysfunction, Dr. Charles Runels sees a widening gap between the medical remedies for men and women — and medical education is partly to blame. https://t.co/FGLM0ebdYu
— Medscape (@Medscape) September 25, 2024
Author: runels
-
The Gap
-
How to Have a Healthy Holiday
Made this one over a decade ago. The tools have changed but the ideas work better than ever. Hope it helps you.
Sincerely,
Charles Runels, MD
-
Female Sex Muscles
All right, thank you for coming to the journal club regarding the female orgasm system. Last week was a disaster, so thank you for showing up again this week. I had some technical problems with presenting our research. But today I want to go into detail and try to make sense of this. Since in not just naming the parts. You can lift the hood of your car and you can name the parts. There’s the carburetor, there’s the, I don’t know, pick something else. You can take off the cover of your computer and say there’s the integrated circuit, that’s a diode, that’s a resistor, that’s a wire, but that doesn’t really mean you know how all those parts work together to make your computer present what we’re doing right now. So your computer is a system and then there are systems within the systems. So the body is a massive system with subsystems in it. And we’re talking now about how the muscles of the pelvis contribute to not incontinence, to sexual function, not incontinence to sexual function.
And as I go, feel free to put something in the chat box, I’m looking at that, not the question box, but put something in the chat box, that way others can see it if you have comments or questions and I’ll promise to get to them before the end. The idea is to make sense of this relate it, not to naming parts, but to functionality in regards to sexual function and relate it to some of the relevant research. So let’s start with some of the parts and how they’re related to what we talked about regarding the clitoris a few weeks ago. Now, this is a nice model, but I have another model that I think helps you see it better. So this is the inside, most people would call this the pelvic floor, but there’s more to the pelvic muscles than the pelvic floor. So before I pull out the other model, just notice that you can see muscles on this side that you don’t see on the other side. You see superficial transverse peroneal muscle, deep transverse peroneal muscle, ischiocavernosus, and bulbospongiosus.
Those are not part of the pelvic floor. I think some people think every muscle down here is if it’s in the female pelvis part of the pelvic floor. Nope, it isn’t. Here you’re seeing the underbelly of the floor where you have puborectalis, iliococcygeus, ischiococcygeal and coccygeus. So those three together, these first three form the really the levator ani. And you can see how if these contract, it’s going to pull the anus up, levator ani. Well, let me pull out the other model because I think it makes it more apparent for you. Okay, so this model has some of the organs in place and when we talk about the muscles of the pelvis, remember of course, there are muscles … we’re going to take out the out the ovaries, the fallopian tubes, and the uterus. But of course the vagina has at least muscle cells in it. And so we’ll put that aside for now. And then let’s take out the bladder, which also has a muscular layer and urethra. The urethra or the urinary sphincter has really three layers, two layers of striated muscle and one layer of smooth muscle.
And some of those layers go circumferentially around both the vagina, so it sits like that. And so some of the muscles go that are more distal from the bladder go circumferentially around both the urethra and the vagina. And then as you get more proximal to the bladder, they just go part of the way. And then you have muscles that go around just the urethra, both circumferentially and longitudinal. But those are, I think, more easy to understand what they do. Now, we have the pelvic floor exposed and you can look through, this is called the hiatus. Wait, let’s pull out the rectum. Okay, so now you have holes in the pelvic floor. You need them, right? So you need a hole for, if you look at the other side, it makes sense, you need a hole for the rectum, hole for the vagina, hole for the urethra. And those would be the hiatus or the absence of the pelvic floor muscles.
So you have puborectalis that comes down. And let’s pull it this way so you can see it better. I’ll hold it more still. I Know it’s jumping around a lot. So you got puborectalis right there. Pubococcygeus comes down right there, iliococcygeus, ischiococcygeus or coccygeus, all of these forming the floor. But look what happens. Now, there’s in reality, in the women, of course these muscles are adjacent to each other. And if you look at the other model, it demonstrates … thanks to my amazing wife, I’ve talked to her about what it’s like to be down there doing surgery and got some of these ideas from her … but there’s not a lot of space right there. And actually dissecting the deep transverse perineal muscle away from the pelvic floor would be difficult because they’re abut each other, but they have different fibers, different functionalities, which we’re getting to and how they relate to the sexual function. So let’s look back in at the pelvic floor. And here’s a question to ask yourself.
If you go with the assumption that there is no redundancy, and no wasted parts in the body, if we put something together … I do it all the time. I put together some stairs for our hot tub the other day and I had an extra part, which bothered me. I don’t think there are extra parts. I guess you could maybe argue that maybe the appendix is an extra part, but not really because it’s vestigial and it’s a part that because it’s extra, sort of dried up you might say, or become pygmy size. So if you go with that assumption, there are no extra parts and every part has a function, then you have to ask yourself. Well, it’s easy to imagine what the bicep muscle does, right, there’s a hinge across our midway in the bicep muscle, and when it contracts, it’s easy to see what it does. It brings the radius closer to the humerus and your elbow acts like a hinge. But if the floor is meant just to hold things in place, why isn’t it a muscle? Why isn’t it just fascia, a thick fascia or tendon or something?
Why was it made to contract and relax? I think that’s a question worth asking. And it gets even more interesting I think. We’ll get to the research shortly, but I think the research makes more sense if you look at the functionality. So we’ve lifted away from the pelvic floor, other muscles, and these are the ones I call the sex muscles because they might contribute to, of course, the anus would contribute to fecal continence. But you could argue the ischiocavernosus isn’t really doing anything for urinary continence that I can see. But now, let’s name them again and let’s think about, well, when it contracts, if there are no extra parts and everything has a purpose, what’s the purpose of this muscle contracting? There’s no joint. This is why I wanted to cover the mystery of the hidden clitoris before we got to the muscle part of the female orgasm system. It’s just so amazingly beautifully designed. I think many of our colleagues just still think of the female genitalia, there’s a tube to put a penis in.
There’s a tube for feces to come out of and there’s a tube for urine to come out of. And they’re not visualizing everything you’re looking at here, but let’s think about it. Okay, so you’ve got labia majora, labia minora, urethra, vagina. Then remember, the root of the clitoris is just above the urethra and it’s all attached. So you’ve got corpus cavernosi. I never know how to say the word crux. Is that crus or cuss or crux or I don’t know what it is, but if you were to say it, I guess say it loudly, so I’m going to call it crus or I think it’s crux, but whatever, corpus cavernosi. So you have two of them that lay along the pubic rami and they’re covered by the ischiocavernosus. And then you have the corpus spongiosus, also part of the clitoris and attached to the root, which is attached to the underbelly of the body of the clitoris. And then you have the glands, clitoris, and that little pink thing right there is Bartholin’s gland. Now think about this.
So what’s the purpose of corpus spongiosus and ischiocavernosus and what’s the purpose of transverse peroneal, deep transverse peroneal, superficial and peroneal body? And so what, even if you can name them, so what, how does it help you have better sex as a female, both for your pleasure and for your psychology, right, because it’s not just about sexual pleasure. I’m not going to start ranting about that, but never forget sexual pleasure is not just about pleasure in the bedroom. It has studies over and over again, somewhere between 30 and 40% of women have psychological distress because of sexual dysfunction. Ever have a cracked window in a nice car, you don’t really need it, it’s not leaking water, but it bugs you. Now, imagine you have a dysfunctional vagina. Even if you’re not using it with your husband, it still bugs you. Even if you don’t want to a man in your house, it might still bother you because you want to make love to yourself.
So I know that’s a sidetrack, but I just never want to forget, this is not just about pleasure, although it is, it’s not just about pleasure, it’s not just about making babies, although it is, because what brings pleasure to the woman is going to bring pleasure to the man if this is designed properly. Think about it. If this is designed properly, this is going to make the man orgasm or ejaculate. So if he wants to again, if we’re looking at it from propagation of the species, from a Darwinian standpoint, then you want this little device to make the man ejaculate. And then because it feels so good, he’s going to want to ejaculate again in a few minutes from now and increase the chances of survival of the species. And then if it feels good to the women, even if he’s in refractory period, if you’re living in a cave somewhere where you haven’t bumped into a period of bulls yet, you might want to have sex with his friend because it felt so good.
Watch the pussycat in your backyard, she’ll have tomcats lined up back to back and she enjoys it. And you know that because she doesn’t run away. Anyway, so I got sidetracked again, but not really because it’s important. Some people say, “Well, you’re talking about vagina, like it’s tighter so it feels better to men.” Oh, no, no, no. Sometimes tighter isn’t better to a man. We never say tighter, loose, looser, big or small, we talk about fit. Does it fit? Actually, the man loses about 50% of the inaudible 00:14:19 of his penis by the time he’s 65. So his penis is shrinking. And now imagine the woman’s delivered several babies, think about what happens to this device when she delivers a child. All right, so let’s go back. I’m just sidetracked, but I just wanted to put this in perspective about why we are talking about this. There’s propagation of the species perspective, there’s pleasure to the man. Don’t deny it because that’s necessary for propagation of the species. And then there’s also pleasure for the woman, both physical and psychological pleasure.
And most of your colleagues, if you’re a physician, can’t name all these parts. All right, so here we go. Peroneal body or the superficial transverse peroneal muscle, deep transverse peroneal muscle, and bulbospongiosus, ischiocavernosus. And there are no joints in that. In the face, the only muscle I know of that is not attached to a bone is orbicularis oris muscle. For a little joke, you can tell your friends, another definition of the kiss is the anti juxtaposition of two orbicular oris muscles in the state of contraction. But the orbicular oris muscle does not connect to a bone, it connects to muscles only. You can say the same thing about the peroneal body. And then you think, okay, what’s it doing? Because when it contracts, there’s no joint moving. And I don’t have a good answer for you, but here’s what I’m thinking is happening. Both in men and women, parasympathetic system causes erection and blood flow in the clitoris. But with ejaculation in men and with orgasm in women, you have contraction of muscles. And so I don’t really know, somebody needs to do the study.
Does the muscle relax and then it contracts with orgasm or does it just contract? Does it contract just with arousal? Another way to think about this and what it’s doing on the first level order of understanding, is just imagine what would happen. Let’s pull the whole thing back up here again. I like to understand something. I like to imagine the extremes. So if this became extremely relaxed, like a worn out rubber band. If all these muscles became like that, superficial transverse peroneal muscle and deep transverse peroneal muscle, if it became relaxed, so there was no tensile strength at all to it, well then with sex, this is not attached to a bone, the introitus is just free floating, right? Of course there’s tendons on the other side, but this is mostly free floating. So when this becomes contractile, it helps hold the vagina in place. And then when the corpus spongiosum and the ischiocavernosus contracts, it would squeeze blood flow, rhythmically if there was orgasm going on, from the corpus cavernosi up into the body and the glands causing congestion and increased arousal.
And so there’s a positive feedback loop. You’re aroused, you have an orgasm, and then with the contractions there becomes even more arousal, more pleasure. And so you want to play again and eventually you make a baby or you make a deeper, more interesting relationship with your lover. Okay, so I’m calling these the female sex muscles. Now, we’ll get to what you can do to make things better. Let me catch up. I’m going to look at my notes, make sure I’m not forgetting anything here. Let’s see, I got that. I want to make sure I cover all this stuff. Okay, let’s look at the research. I think I’m at a good place now to do that. We may come back to the model, but let’s look at the research. Oh, I know what I’m going to show you. So remember one of the studies we looked at involving the clitoris. Even though the clitoris has the most no fibers, their understanding, Dr. Paul’s, if you remember, was that the root was the most arousing. Now, think about that.
That actually coincides with Dr. Gräfenberg’s idea about the urethra, which eventually evolved into the G-spot named after Dr. Gräfenberg. So if you go inside the introitus and you push up, you are then putting pressure on both the urethra and the clitoral root if you’re just inside the introitus. Now, once you get past these muscles, what I’m calling the sex muscles, into the vagina itself, the strength goes down. Now, watch a man when he masturbates. There is an increased pleasure if there’s a wave of compression. In other words, there may be more compression on one part of the penis and then that compression moves up and down, which is exactly what would happen if these muscles were contracting. In other words, if the introitus was tighter than what’s going on inside the vagina. Okay, let’s look at the research. Some of that was me going by common sense. Some of it was based on research. Some of it I might’ve just made up because it sounded good, but I think most of what I said was right. Okay, let me show you some other stuff.
Remember what William Ocer said. He said, “If I ask three medical students how long it takes for the fingernail to grow, one will not give it a second thought, another will look it up in the book, and the third will take a silver nitrate stick and put a mark at the base of their fingernail and see how long it takes to grow to the end.” So I think I’m dealing without those sorts of students here on this call. We’re all students trying to understand what has not been explained adequately and deserves much more research. Okay, let’s look at some of that research and then I’ll talk about some of the actual things we have, the technologies and ideas we have to actually make these muscles work better and deal with the dysfunction that might happen. Okay, hold on a second, let me show you something else. Okay. Here we go. My grandmother used to have a saying that I was reminded of when I read this research. She was a sweet lady who was a little quirky.
She had a Jesus picture on every wall, but never went to church unless somebody got married or died. And she’s the only person ever knew in my life who I never heard in my entire life ever say anything bad about anybody, like nobody else I can say that about. And she used to tell me, “Charles, if you go outside and you sprinkle a little salt on a bird’s tail, it won’t be able to fly away and you can catch it.” If you think about that, it’s the old catch 22, right, because if you’re close enough to put salt on the bird’s tail, well you are close enough to catch it without the salt. And this study reminded me of what my grandmother used to tell me. So let me show you what I mean by that. So what they did was they took women and they had them do the Kegel. And when they did the Kegel, they looked to say, I’ll just show you. So they did bi-digital palpation, so two fingers, index and middle finger. They even said which fingers, into the vaginal introitus, about four centimeters in.
Okay, let’s get our … well you can remember the model, but you just saw it so it’s in your head. So you go four centimeters in or a little bit less than two inches. And then they instruct the woman to squeeze their levator and anal muscles without activating other groups of muscles. In other words, you can’t contract your gluteal muscles or your legs or your abdomen. Then they palpated pubococcygeus on each side of the vagina and said, “Do a maximal contraction of the pubococcygeus.” Okay, now they scored it. I’m getting to the part about the salt on the tail of the bird, promise it relates. So then they scored it from a grade zero, no contraction, grade one minor flicker, grade two is a weak muscle contraction, grade three, they’re only really starting to feel it, grade four is good and then grade five is strong. Okay. So grades one through five and zero is nothing. One’s a flicker. Not until you get to three do you really actually have something happening.
And if you look at what they snuck in on you is they basically defined that one muscle, a pubococcygeal muscle with the pelvic floor muscles. And as you just saw, really is a lot more there, but okay, it’s a good way. It’s easy to reach with your finger, easy to identify, you just put your finger in the vagina, feel over to either side and that’s it. Now, here’s the interesting part. When they graded them on female sexual function index. I love this study. They looked at it and they saw, as you would expect, those with a stronger muscle had better sex. But here’s the part about the salt on the tail. Now, what do you do with that? Oh, let me give you a link to this because some of you guys are going to want to read this study. Hold on a sec. And it will be definitely be out when I send out the PDF file of this webinar. Hold on a second, I’m distracted because I’m clicking buttons. Okay, there you go. There’s a link to the study.
But here’s the thing, okay, let’s just think. Great, stronger muscles, well, that’s what we need to do because that’s going to lead to better sex. Here’s the catch 22. If you have a weak or a flicker, how do you exercise something you can’t move? And the women who could actually do that … So let me put it a different way. I want you to build up your bicep. Here’s a dumbbell. Now, do some dumbbell curls but you are unable to move your bicep. There is an answer and I’m getting to one of those answers. And I realized with some coaching, even a flicker could be eventually coached up into something stronger. But I’ve got a way to maybe do better than that and I’ll get to it in a second. Hold on a minute. Here’s another one, strength and bioelectrical activity of the floor. There’s so many pelvic floor muscle studies out here. And they verified that primary outcomes or level of strength, pelvic floor muscles and then measure biological activity and sexual function and related it to both stress incontinence and sex. And what do you think?
As you would expect the people who had weaker muscles and stress incontinence, those with stress incontinence have lower sexual desire and bioelectrical activity with the correlated parameters. Lower pelvic floor muscle strength impacting the worse severity of urinary loss and the relationship between the domains of sexual function were all involved except for desire. So now, and I’m just going to drag all of these references over into the chat box while I’m thinking about it and I won’t have to keep clicking. This will go away now when I close the webinar, but if you copy paste it now, you’ll have it when the webinar is over. So here’s another one. Effects of pelvic floor muscle training on sexual function and satisfaction. Conclusion, pelvic floor muscle training, effective improving sexual dysfunction and satisfaction of urinary symptoms. Now, remember pelvic floor, when you do a Kegel, remember those sex muscles I was showing you, ischiocavernosus, superficial and deep transverse peroneal muscle and bulbospongiosus, that is not pelvic floor.
So let me put it to you a different way. If you’re a female right now, close your eyes, concentrate real hard and contract your ischiocavernosus. Got it? Now, contract your bulbospongiosus. If you had trouble thinking about how to do that, well, so would everybody else on the planet. So what could you do? There’s another one. And you realize these are just samplings, there is so many freaking studies out there. Do we really need another one? Pelvic floor muscle training can improve sexual function, whatever we’ve known it. We’ve known it for probably 20, 30, I don’t know, when did Dr. Kegel think of this exercise? I’m embarrassed I don’t know the history of that, but I’m thinking it’s about 40 years ago. All right, so what’s new under the sun? What can we do? And let me make sure I’ve showed you everything about that. And then I want to get to things we can do, things that can go wrong, and things we can do to treat it. I think that’s all for that. Let me swap back over to my picture and let’s think about things to do to treat it.
Okay, so in that study, when they talked about pelvic floor muscles and they could feel either a flicker or nothing at all, in those who had lesser degrees of sexual satisfaction, they were talking about puborectalis, that’s what they were palpating. And you can see your finger goes in, you just feel to the side, your on puborectalis. No, what are some things that can go wrong? One of them is you can get dyspareunia from pelvic floor, just like you can get a muscle spasm or a tear or an injury to your back. You can have problems with the pelvic floor. Imagine a 10 pound baby blasting through that hiatus, as they call it. And then what’s going to happen to these muscles? They’re not as big as your bicep. And then there’s sexual trauma and then there’s just being alive. Your valsalva when you have bowel movement, or you ride your bicycle and you fall down, or you climb your cliff, if you’re a rock climber woman, and things get injured. Here’s another basic principle I think is worth noting.
If you want ideas about how to treat something, excuse me, one way to get some clues is to look at what are they doing with athletes that make a hundred million dollars per year or race horses that sell for a hundred million dollars. And if you look at that science, or if you just think about, I don’t know, high school, if you’re a high school athlete, male or female, high school athlete, what did you do? You had physical therapy with massage and vibration and strength building with contraction and relaxation. You had pressure points and you had nutrition. And then if you had a really bad tear, you might immobilize it or you might do a trigger point injection with corticosteroids. Now, think about what happens. So if you look at what’s happening now with … Oh, I got to show you this paper. I didn’t show you this paper. I’m going to show you one other paper because it relates to what we’re talking about. It’s in your handouts, but I want you to see it because this is so huge.
If you are a $100 million quarterback and you tear your thigh muscle, I promise there is one thing that you’re going to get that you probably did not get when you delivered your baby. And I’m about to show it to you. Let me put that a different way. There’s probably something that you did not get when you delivered your baby, but it’s routinely done. So when you injured your muscles delivering a child, in my opinion, you got lesser use of available technology than what a quarterback gets, even a college quarterback, when they injure a muscle or a tendon. This is a recent study, you can see this one came out this year, showing how platelet-rich plasma because of growth factors that activate pluripotent stem cells to grow new tissue was used to heal a tendon tear. And there are hundreds of studies like this in the sports medicine literature regarding muscle repair. Let’s see if I can pull up a few of them. Let’s see.
I have some representative ones here. Here we go. Here’s a few of them regarding muscle repair. I’ll throw these in the chat box too so you can copy paste them. But what happens if you don’t inject PRP and you tear a muscle, and we know this because again … I hope this makes you angry, it aggravates me. Should it at least aggravate you or you’re on the wrong call … if you tear a muscle in an elite athlete and then it heals, there’s fibrosis, there’s loss of strength, could be loss of function, and the healing time can be prolonged. And if you miss a day of work and you’re making a $100 million a year, then whoever’s paying your salary doesn’t like it. So what do they do? They inject it with platelet-rich plasma and studies show that activates stellar cells or pluripotent stem cells and you avoid this. You don’t have as much fibrosis, you recover your strength faster, and you avoid dysfunction of the muscle that was torn whether it was the thigh muscle, back muscle, whatever was injured.
So back to what we’re talking about, this is just one and I just copy pasted other representative studies. So one thing that you can do to help with recovery would be just good nutrition. So you have healing. You could have massage, which could be pleasant. You have a pelvic floor physical therapist just like you have a … and again, I’m just thinking analogies between quarterback for the Dallas Cowboys, mother who just delivered a child, or mother who delivered a child 20 years ago and now she’s postmenopausal and trying to recover the muscles that were damaged or atrophied some with time. And those studies have been taught just like a man’s bicep atrophies, a woman’s pelvic muscles atrophied. Notice I didn’t say pelvic floor, pelvic muscles including those transverse peroneal muscle, et cetera. Okay. So you could have physical therapist. You could have cortisone if you had a tear, but you would never do that to a quarterback, although, it’s still being done for pelvic floor tenderness in regarding to dyspareunia in women.
But if you’re a quarterback, you would never have that done because you’re going to have atrophy. Even in the joint it’s been found that you’ll have immediate pain relief if you do inject joints with cortisone. But if you watch the joint over the course of a year, you have less joint destruction and even repair with platelet-rich plasma where you have continued atrophy or even acceleration of osteoporosis and degradation of the joint when you use cortisone. So why are we still injecting pelvises with cortisone instead of with platelet-rich plasma as is done if it’s the muscle of an athlete. A muscle is a muscle is a muscle. I don’t know, but thankfully you’re on this call and you can help us change that. So now, what do you do? So you’ve got massage, which could be your lover, it could be yourself. You got trigger point release and there’s a whole science there.
Your pelvic floor physical therapist could do it. But now that you know the anatomy, you can think about what you could say or do, tell your lover to do or do for yourself if you wanted to release tension in the pelvic floor or one of these other muscles like transverse peroneal, superficial or deep or your peroneal body. So you got trigger point release, you could do acupuncture. All these things are done with athletes. You could do vibration, that could be fine. You could also do heat or ice, both of those things are used. And then platelet-rich plasma we just talked about. Now, where would you find somebody to do platelet-rich plasma … and I’ve got one other thing … for the pelvic floor. We’ve been doing it for a decade now, more than a decade, 13 years we’ve been doing a modified O-Shot where we do, you can still have PRP into the anterior vaginal wall, but you can also … and I just Googled, this is our directory. I just Googled and all these people have been certified by taking some sort of test after training and properly licensed and understand our protocols.
We have about, I don’t know, 1,500 of them, but there’s 30,000, 35,000 gynecologists, 20,000 urologists in the US. We need more people who know how to do this, so help us spread the word. But the people in this group, I just Googled California to give you a representative sampling, know how to find, not just inject anterior vaginal wall and clitoral body, but find trigger points in the pelvis and inject there as well. And I think, thinking about this, there’s going to be a modification as well that involves injecting the peroneal body with platelet-rich plasma, easy to find, easy to palpate, and that would increase strength of ischiocavernosus and bulbospongiosus as well as superficial and deep transverse peroneal muscles. Now, the other thing we remember we talked about what do you do for the woman who can only flicker or do nothing? How do you train that muscle? It’s like catching a bird with a salt on the tail. If she can move the muscle really good, she wouldn’t need to train it, but since she can’t move it at all, she can’t train it. So she’s caught.
Well, that’s where your Emsella machine comes in and there are other devices, I think this is probably the Cadillac. And they don’t pay me any money to say that. There used to be a vibrator called an Intensity they called muscle contraction. I’ve heard it’s gone out of production, but even that was not as powerful as a fricking Emsella machine. And I’ll show you what it looks like. But if you’re going to use it for sexual function versus urinary incontinence, you should modify the way it’s done. And if you talk to one of our people, if you go to the O-Shot directory, those who have an Emsella machine, it costs as much as a house, so most people don’t have one. But if you find someone who has that icon by their name, then they not only do the O-Shot, but they could combine injecting the pelvic muscles, not just the pelvic floor but the pelvic muscles with PRP along with the O-Shot for sexual function and urinary incontinence. And the Emsella is a Tesla magnet that causes contraction.
So here’s their website, but it causes contraction. They’re showing contraction of the pelvic floor, but I’m about to show you how to modify the way it’s done and people in our group will know how to do that … You see, there’s a picture of what we just got through talking about … how to modify the way that’s done so that you are contracting not just pelvic floor, but the female sex muscles. Okay, so I think that’s all I had to say. Let me look at that. Okay, so the ideal treatment or the Cadillac treatment could be for sexual enhancement or correction of dyspareunia. For dyspareunia in the pelvic floor, it could be injecting platelet-rich plasma with a modified O-Shot by one of our providers combined with pelvic floor physical therapy combined with good nutrition and go have sex. I love part of our aftercare instructions are usually go have sex. But it should be one of our people so they know how to do that properly. It’s not just a freaking shot. People need to know how to make the plasma correctly, how to activate it.
It’s not just throw that needle up in there anywhere. You can hurt people, not damage them, but you can make them hurt. You can cause pain and if you don’t know what you’re doing and preparing it, you could unsafe. So our people know how to keep it safe. And our people offer money back, they’re not going to keep your money if you don’t get better. We’re not stealing from people and not going to treat you if they don’t think they can get you better. Okay. So that would be one modification for pelvic floor tenderness with dyspareunia. The other modification for just a super enhanced sexual enhancement could be improving orgasmic function or arousal, could be what we already know. Remember, I don’t have to prove this, we know it, that exercising the pelvis, I just showed you one of literally hundreds of studies showing exercising the pelvis leads to better sexual function.
And then I showed you studies showing that injecting platelet-rich plasma leads to enhanced and improved muscle function and now you’re combining improved muscle function from the exercise physiology research with muscle function with the Emsella, and then you go have some good sex and combine that with just good relationships. Never forget that’s an important part of the female. All the rest of the female sexual orgasm system applies. All of it, endocrine, the brain, the spinal cord, the clitoris, the urethral tract, all the stuff. Some we’ve covered and some we haven’t, still applies. But I think with that, unless there’s questions, we will call it a day. Let’s see what we got. No questions. So hopefully that’s helpful. Eventually I’ll send the PDF transcript out of this that’s edited and tightened up some. And I hope that if you are a patient or a physician, that you found something helpful here to make life better. Have a good day.
-
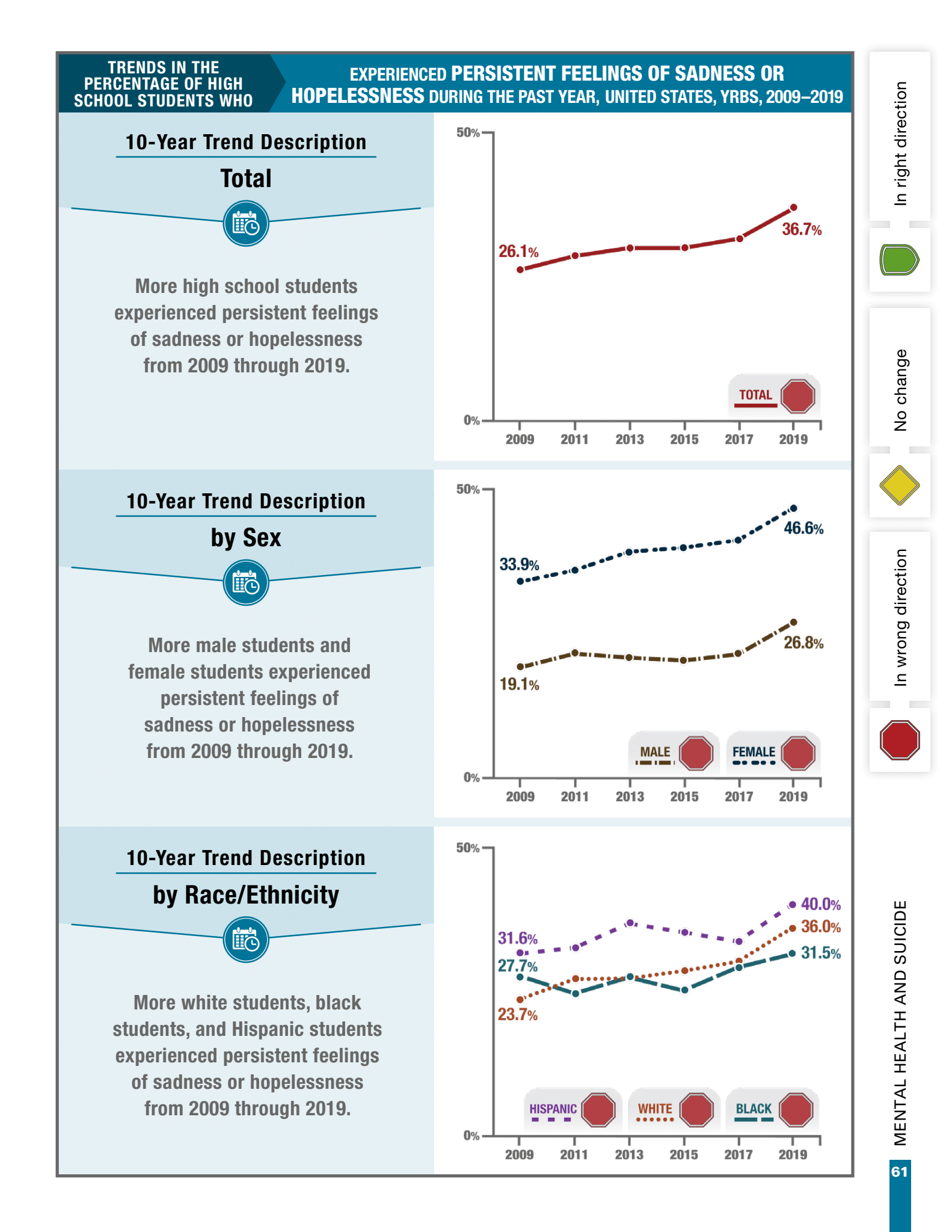
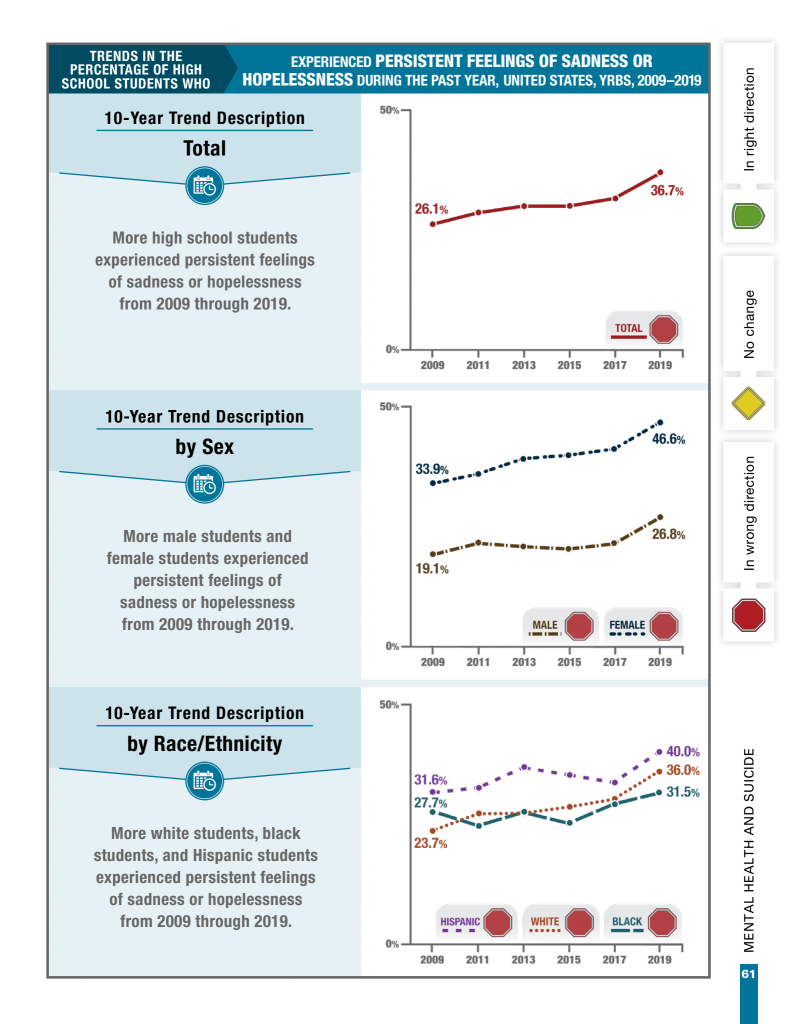
Youth Risk Behavior Survey by the CDC
The Youth Risk Behavior Survey by the Centers for Disease Control (CDC) offers insight into mental health, sexual behavior, and substance abuse practices.
Notice that depression went up by 10% in teens from 2009 until 2019. And, it has gone up even more since then.
-

COVID Vaccine Disinformation (please read and share for the benefit of our families)
If you follow my emails, you know I’ve not agreed with all of the policies of the CDC regarding COVID (based on the numbers publically available)
This very important article delineates the facts regarding COVID vaccination:
For your examination…COVID Disinformation<–click to read<–I hope you will share, mostly not for changing COVID policies; what is more important than COVID, in my humble opinion, is the seeming lack of desire (even among, maybe especially among, young college students) or courage to question (not necessarily disagree, simply to question) authority and the severe consequences of questioning authority that was real and is real.
Science becomes impotent and even destructive when scientists become afraid to speak.
There can be no free thought, no virtue, no advancement of science without courage.
Charles Runels, MD

-
Priapus Toxin™ & P-Shot 100™
Outline
- The Priapus Toxin™ and P-Shot 100™ procedures
- Scientific research regarding Priapus Toxin™ and P-Shot 100™
- How to schedule an appointment
The Priapus Toxin™ and P-Shot 100™ Procedures
We have now been doing the P-Shot® procedure for over ten years with much success and with a significant body of medical research supporting the procedure.
Over the past six years, a growing body of research (in animals and people) also supports the effectiveness and safety of injecting the corpus cavernosi of the penis with BOTOX. In the latest randomized, double-blind, placebo-controlled prospective comparative study, the most effective and longest-lasting dose for improvement of erection firmness was 100 units of BOTOX, in total (50 units into each corpus cavernosi). This dose showed effectiveness up to 6 months with maximal effect at 6 weeks.
The mechanism of action of botulinum toxin in the penis seems to be partly due to the relaxation of the smooth muscle of the arterioles, resulting in increased blood flow (and even a small increase in length in one study). This increase in erection firmness by increasing arterial flow is exactly how Viagra and Tri-mix injections work. In two separate studies, the injection of botulinum toxin was helpful to some men (not all) for whom Viagra and Cialis had quit working.
Botulinum toxin (at doses much higher than 100 units) has been used for two decades for various problems with an extremely safe history.
The P-Shot 100™ (Priapus Toxin™) procedure is a specific method of injecting blood-derived growth factors, including platelet-rich plasma (or platelet-rich fibrin matrix) and botulinum neurotoxin, to improve the health of the penis and enhance the size or function of the penis. The procedure includes patient selection, method of preparation of materials, method of injection, aftercare, and more.
I am now offering the P-Shot® (Priapus Shot®) procedure combined with 100 units of Botox–the combination of the two is called the P-Shot 100™ (Priapus Toxin™) procedure.
Suppose someone wants Botox alone injected into the penis. In that case, we have the Priapus Toxin™ procedure: a specific method of injecting the corpus cavernosi of the penis with botulinum neurotoxin (BoNT)–BOTOX– to improve penile tissue health and to enhance erectile function or penis size. The procedure includes patient selection, the method of preparation of the botulinum toxin, the method of injection of the botulinum toxin, aftercare, and more.
As with all procedures, there can be no guarantee of the outcome (though I do guarantee not to keep your money if the procedure does not meet your expectations), and there can be complications (some unexpected and of unknown severity). Using Botox for ED is an off-label use for BOTOX not approved by the FDA--as are other common "off-label" uses of BOTOX. Some experts do not think Botox should be used for ED. Thankfully, we have 2 decades of use of Botox, with millions of doses per year, for many indications with an extremely high safety profile. The toxic LD50 for injecting cosmetic Botox iv for a 180-pound man is estimated to be around 150 to 200 Bottles of Botox (or around 15,000 to 20,000 units); we only inject a total of 100 units of Botox (one bottle) into the corpus carvernosi when we do the procedure (a smaller dose than what is often used to treat children with muscle spasm).Guarantee: If you are not pleased with the results of your procedure for any reason or no reason at all, you can get a full refund for the procedure for up to 6 months.
Scientific Research
- Abdelrahman, Islam Fathy Soliman, Amr Abdel Raheem, Yaser Elkhiat, Abdelrahman A. Aburahma, Tarek Abdel-Raheem, and Hussein Ghanem. “Safety and Efficacy of Botulinum Neurotoxin in the Treatment of Erectile Dysfunction Refractory to Phosphodiesterase Inhibitors: Results of a Randomized Controlled Trial.” Andrology 10, no. 2 (2022): 254–61. https://doi.org/10.1111/andr.13104.
- El-Shaer, Waleed, Hussein Ghanem, Tamer Diab, Ahmed Abo-Taleb, and Wael Kandeel. “Intra-Cavernous Injection of BOTOX® (50 and 100 Units) for Treatment of Vasculogenic Erectile Dysfunction: Randomized Controlled Trial.” Andrology 9, no. 4 (2021): 1166–75. https://doi.org/10.1111/andr.13010.
- Giuliano, Francois, Charles Joussain, and Pierre Denys. “Safety and Efficacy of Intracavernosal Injections of AbobotulinumtoxinA (Dysport®) as Add-on Therapy to Phosphosdiesterase Type 5 Inhibitors or Prostaglandin E1 for Erectile Dysfunction—Case Studies.” Toxins 11, no. 5 (May 21, 2019): 283. https://doi.org/10.3390/toxins11050283.
-
Habashy, Engy, and Tobias S. Köhler. “Botox for Erectile Dysfunction.” The Journal of Sexual Medicine 19, no. 7 (July 2022): 1061–63. https://doi.org/10.1016/j.jsxm.2022.03.216.
-
Naumann, Markus, and Joseph Jankovic. “Safety of Botulinum Toxin Type A: A Systematic Review and Meta-Analysis.” Current Medical Research and Opinion 20, no. 7 (July 2004): 981–90. https://doi.org/10.1185/030079904125003962.
How to Schedule an Appointment
If I speak with you by phone after you schedule your appointment or even during your initial visit, and we determine the procedure may not be the best choice for you, then you will receive a complete and cheerful refund. You will not even be charged for the consultation.
— Charles Runels, MDP-Shot 100™ (Priapus Toxin™)
The P-Shot® procedure combined with the Bocox™ procedure (PRP combined with 100 Units of BOTOX).
$2,787
Schedule here<–Priapus Toxin™ Procedure: botulinum toxin 100 units alone (no P-Shot® added) injected into the penis (50 units into each corpus cavernosum)
$1,797
Schedule here<–
P-Shot® (Priapus Shot®) Procedure: The first procedure.
$1,800
Schedule here<–Repeat P-Shot® (Priapus Shot®) Procedure: Repeat injection (recommended to wait 8-12 weeks for the full benefit of the first injection before determining if a second injection is needed)
$997
Schedule here<– -
Altar® Club
Buy one bottle for $97

Subscribe for $92 per month
-
It is not your imagination–Botox really does help make you happier
The Need for New Treatments for Depression
(Research references for this article are listed at the bottom of the page)
Three hundred million people worldwide suffer the physical and mental pain of depression. And according to the World Health Organization (WHO), depression is the leading cause of disability worldwide. (Whitcup2019)
Everyone has someone close to them who suffered depression to the point that it interfered with life in a significant way. And because a large portion of people does not respond completely to our current therapies, millions of people suffer chronic depression. (Whitcup2019)
In other words, we need something that works better than our current therapies.
Recently, a review article, which covered the past two decades, showed that even though serotonin reuptake inhibitors improve the symptoms of depression for millions of people, they also increased the risk of suicide, and (surprisingly) the article also showed that the whole idea of a “chemical imbalance” of serotonin in the brain causing depression is wrong. (Moncrieff2022) (Wise2022)
If you are currently taking a serotonin reuptake inhibitor (SSRIs), do not stop taking it without the help of your physician--these medications do help many people, and stopping them abruptly can be dangerous.We now know that depression is not caused by low levels of serotonin!
We need a better way to treat depression.
The Biggest Barrier to Something New & Helpful Entering Your Brain
So many of our present therapies for depression (SSRIs) are based on a debunked theory of serotonin imbalance!
That does not mean that SSRIs are not helping many people, but it does mean that SSRIs are not helping the way we thought they do and it explains why SSRIs do not make chronic depression go a way for millions of people.
For us to keep teaching that depression is caused by a serotonin imbalance is like teaching about the tooth fairy; it ain’t what causes depression.
So, something’s happening when you take SSRIs. What is it?
Here, I’m going to tell you my pure speculation—no research to back it up: SSRIs just dull the senses (more about how later in this note). People feel their depression, they just do not worry about it much. Anorgasmia, continued dysphoria, and an increased risk of suicide and maybe homicide (because you would also be less worried about death)—those are the gifts of SSRIs. Perhaps the depression’s not felt as much, but also fear is not felt as much, which explains why people are less afraid to kill themselves.
So, I am not saying we throw away all antidepressants, but we need to get off the idea that we have depression all figured out and we don’t need something better to treat it; because we do.
Also, as an internist, I would never propose a magic bullet. Depression can also be caused by situations, life events, hypothyroidism, low growth hormone levels, malnutrition, postpartum hormone changes, elevated prolactin from pituitary microadenomas, and much more; Botox would not help any of these.
So, Botox is not a magic bullet to cure all depression. Multiple papers and strong science do suggest that Botox be used for depression as part of a multifactorial approach in some people.
But, BOTOX has not been used as standard therapy for depression partly because we thought we knew that low serotonin was the problem; so how could BOTOX help?
Well, serotonin is NOT the problem, but most doctors still think it is and so think BOTOX for depression does not fit the model—so they do not use it.
In short, the hindrance to knowing something new is not ignorance, it is the illusion that we already know the answers, so we don’t need something new.
We must get over that; we need something better for the treatment of depression, and we need better combination strategies to treat depression.
So, now consider Darwin to consider a new and strong approach that has reached its time.
Darwin & Depression
Charles Darwin described muscles that express depression.
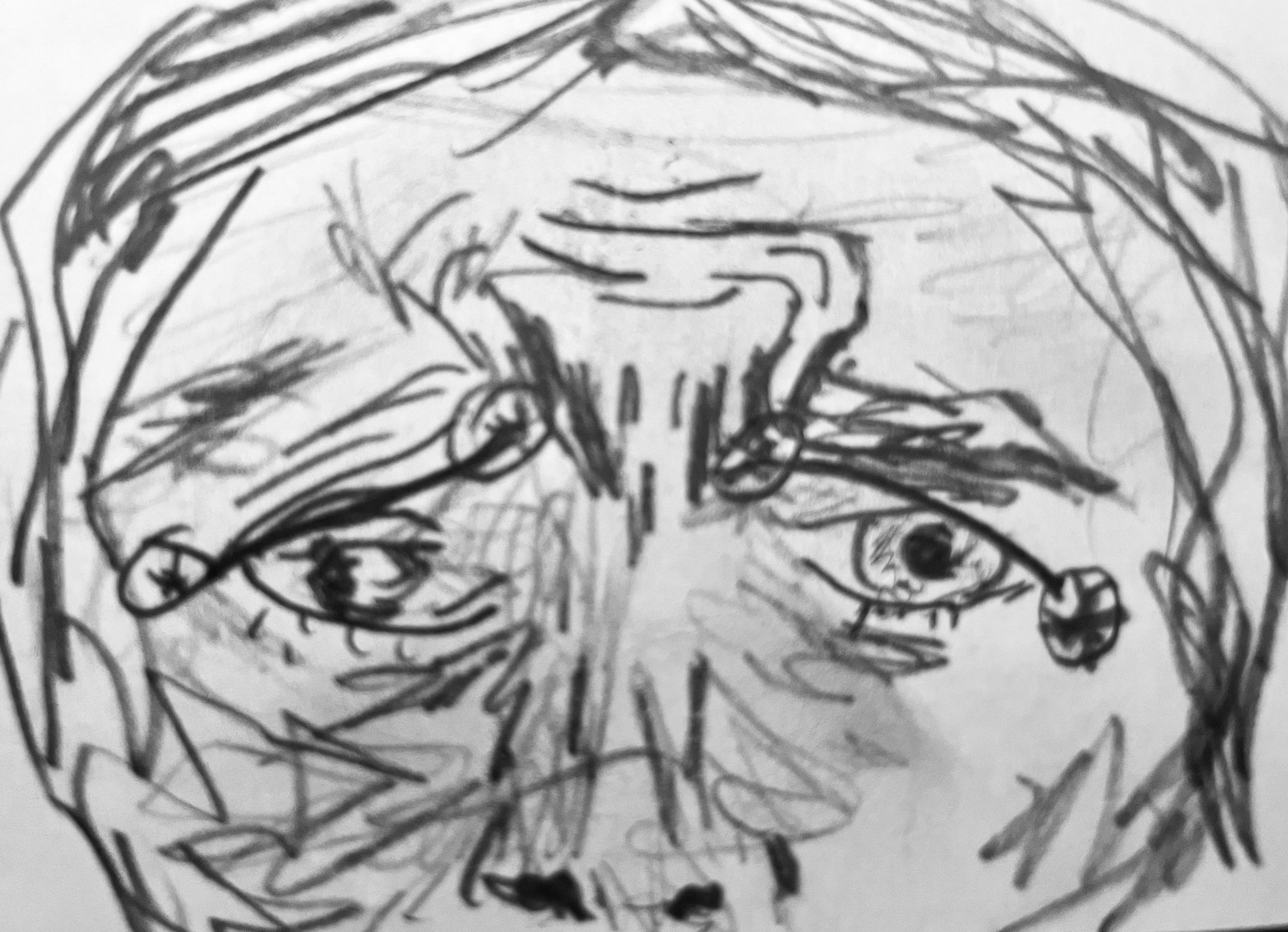
First, there is the omega melancholicum which is the combination of the corrugators and the medial part of the frontalis; when someone is worried, anxious, or sad, those emotions create the number 11 signs (from the corrugators), but also this complex of muscles creates a contraction of the medial frontalis, which completes the omega melancholic configuration—it looks like the Greek letter omega.
If you are depressed, you also demonstrate lines called Veraguth’s folds that go from the lateral corner of the eye to the medial eyebrow.
When you draw out the omega and those folds, you see a face that’s worried and sad and tearful and afraid and depressed.

“Veraguth’s Folds” (*) and “Omega Melancholicum” Now that you see the configuration of muscles described by Darwin and others consider how Botox may be of help.
BOTOX and Depression-How it Helps
Multiple studies show that Botox helps depression (see the extensive references in Whitcups excellent textbook chapter 2019).
Even in people that are resistant to antidepressants, BOTOX can help; and now, you know a possible reason why.
And now we know that not only does Botox help depression in those that are resistant to antidepressants, but it also blocks feedback loops that make depression worse. For example, there was one study that showed that if someone says something to you that should be causing you to be sad or depressed, with Botox, there’s a delayed response just in the perception of it. It takes us longer even to think that’s something sad when we hear it.
The Facial Feedback Hypothesis
One of the theories that have been talked about as a possible explanation of how Botox might be helping depression is called the facial feedback hypothesis.
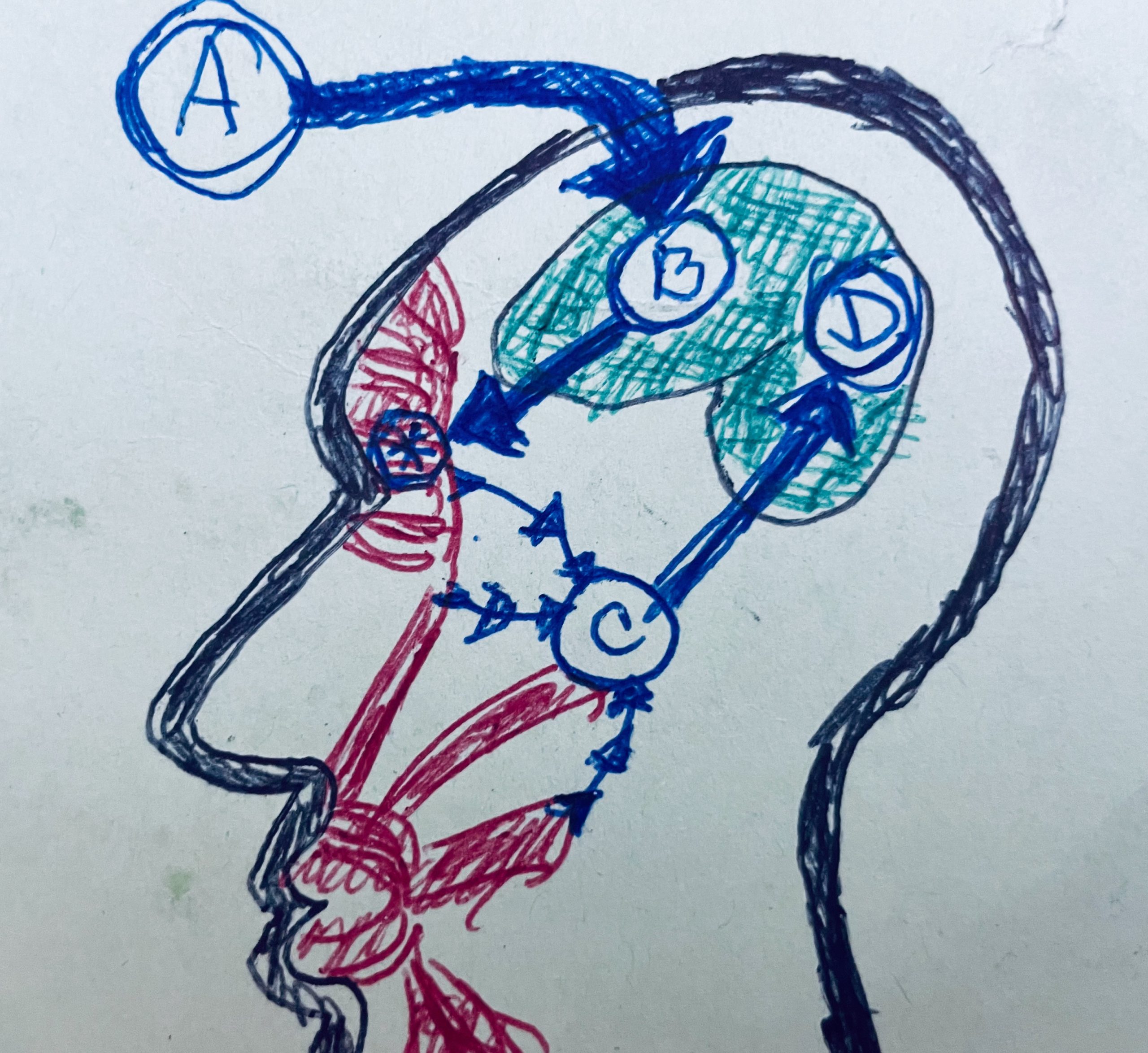
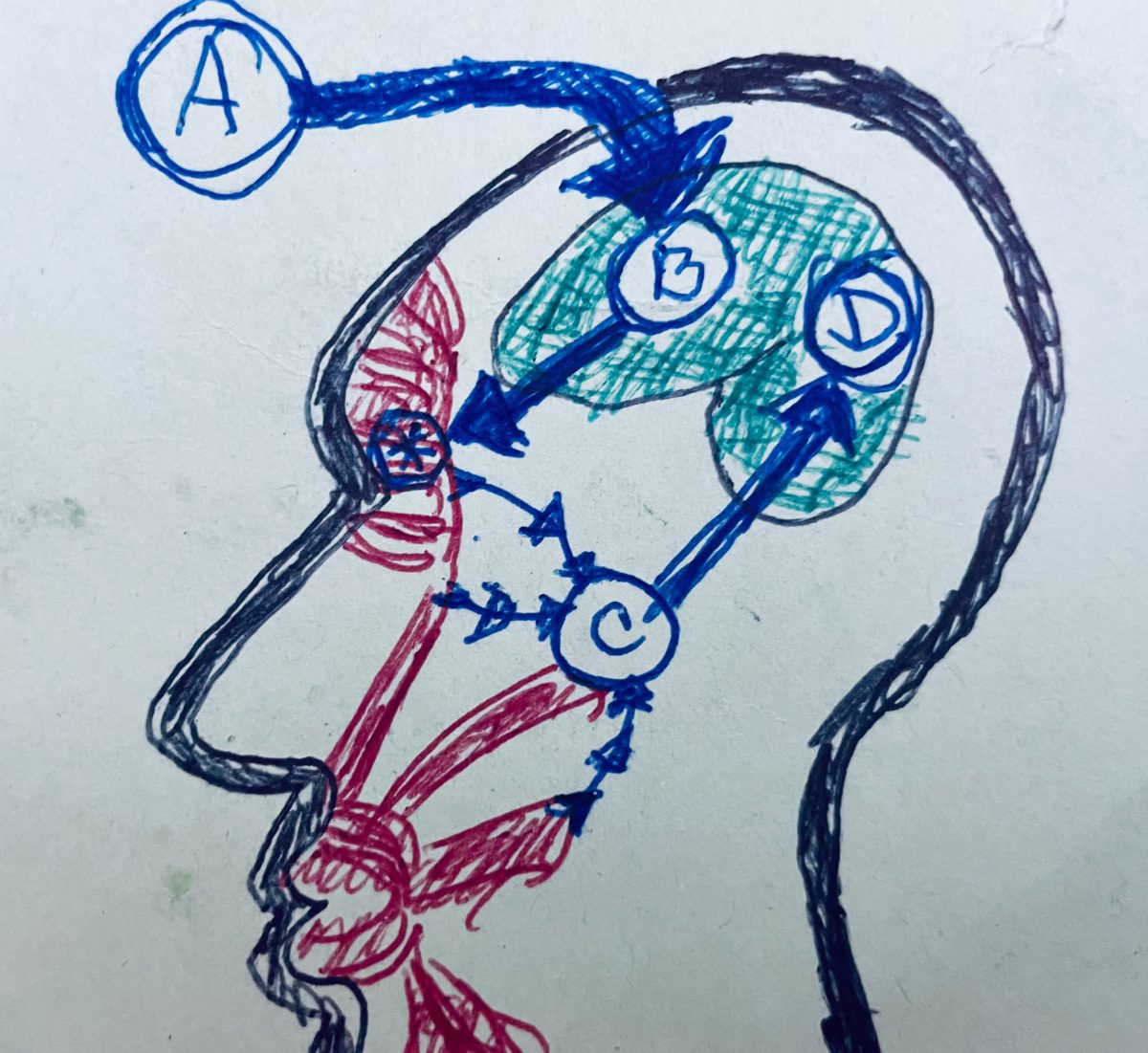
The following diagram shows how it works. (Abdulmohsen2011) (Whitcup2019)
First, you have something coming into consciousness: you hear it, you see it, you think about it; you have this psychological or cognitive information that enters the consciousness and causes what’s called a cold emotion.
So you know about it, but it hasn’t escalated into this visceral thing where you feel like you were punched in the gut—an emotion where you feel heartache, and everybody knows heartache is not a metaphor; your heart aches.
In couples who have been married for over 50 years, the surviving partner bears a death rate after loss of a spouse within a year of the death of their spouse; their heart does not just ache. Their heart breaks, and they fall over dead.
Going from a cold emotion to a warm emotion does not just hurt; it is dangerous. So, stopping the transformation of a cold emotion into a warm emotion is huge (this, in my humble opinion, may also be what SSRIs are doing).
And so (in our diagram of the Facial Feedback Loop), one of the ideas is that once the idea enters the consciousness (illustrated by the “A arrow”), then the “B arrow” perceives it. And it triggers facial musculature activation.
Those muscles that we just described are the main ones that are triggered, the corrugators and the medial part of the frontalis– causing those two configurations, Veraguth’s folds, and the omega melancholicum.
Then the muscles move.
In the diagram of the Facial Feedback Hypothesis, the star with a circle around it illustrates what gets blocked by Botox (the feedback is blocked between C and D).
So the signal to move the muscle just dies, the feedback is blocked, and the emotion stays cold.
But, follow what happens without the Botox: the muscles move, and then C illustrates the proprioception of the movement of the muscles.
So in the musculature, you have nerves that tell the muscles to move.
Then you have nerves that sense that the muscles have been moved. So that’s illustrated by C, the proprioception of the facial muscle signals, the emotional brain, or emotional proprioception.
And then, the emotional proprioception signals enhance the cold emotion and set it on fire into the somatically-enhanced “warm emotion.”
I am not going to keep calling it a warm emotion (as it is called in the medical research). I’m going to call it a pants-on-fire, hot emotion that just burns up your peace of mind.
Think of your peace ignited by C, and then with D, you have not a warm, not a cold emotion like you did with B, but you have D, which becomes a warm emotion or a hot emotion.
Well, guess what happens now?
Facial Feedback Can Cause a Death Spiral
It’s not illustrated in the diagram, but D causes B to tell your muscles to again make the sad face (Omega Melancholicum and Veraguth’s folds)—which goes back to B, which cycles back to D, over and over and over.
Now, you suffer a negative feedback loop that spirals people down—that just can put people collapsed on the floor in tears or vomiting or putting a pistol to their head.
How beautiful is it to have something that blocks that horrific cycle where B does not have the chance to cause that feedback loop?
I am not saying that BOTOX for a grieving widow will make her feel happy. But, BOTOX might attenuate the pain to be bearable and survivable–helping her through the fog to the other side (My observation is that it usually takes a month for every year that someone was married to grieve the loss, in both divorce and death).
Condensed Explanation
When Botox is used in the corrugators, not only do the facial muscles not react to enhance the cold emotions (sadness, anger, and fear) into warm emotions, but also the feedback loop is broken.
IMPORTANT: Because the feedback loop is broken, now there continue to be signals from the face (with Botox use in the corrugators) of calm and happiness–not only blocking the negative feedback but also (by keeping the corrugators relaxed) providing continuing emotional proprioception of peace!
So, the brain may first perceive “sad” (A in the diagram), but C keeps telling the brain, “No, you are not sad, you are at peace; you are calm; you are not afraid; you are not angry.
And that’s what Botox does for you. At least, that is the facial hypothesis.
Speculation…Botox, Depression, & the CNS
Now, what I’m going to tell you is Charles’ hypothesis/speculation about something that would help BOTOX work for depression in ways more than what is implied by the facial feedback hypothesis.
We also know from pain studies (like treating bruxism and migraines) and from animal studies that Botox travels along the axon to the central nervous system and affects this feedback loop centrally.
So, we know there’s also a central effect from BOTOX, not just blocking acetylcholine at the muscle-nerve synapse.
Again, we used to think that Botox is just acting on the acetylcholine receptors so that the nerve cannot stimulate the muscle to contract. But now we know the effects are much more elegant, much more complicated than that. BOTOX helps relieve pain by actually migrating into the spinal column. (Mazzochio2015) (Caleo2018)
So, that means with the treatment of the facial muscles, BOTOX is migrating along the cranial nerves.
So what is that doing?
I have no idea!
But, I cannot imagine that it does nothing–and it could be part of the way BOTOX helps people feel less sad.
But, even though we do not know for sure how BOTXO helps depression, we do know (from multiple studies) that some people who suffer from depression so severe they do not respond to medications are helped by treating the corrugators with BOTOX.
And, we know that their depression is not caused by a paucity of serotonin.
What About Insurance?
So, what the heck are we waiting for?
In my opinion, we should be offering Botox to everyone who is clinically sad and not responding to non-pharmacological measures (I still think 21 miles a week on foot is one of the best treatments for depression). And we now know that BOTOX can help some people who suffer from personality disorders.
It becomes almost an ethical problem to not use BOTOX for depression (assuming none of the contraindications like pregnancy and myasthenia gravis).
So, what keeps us from offering BOTOX for depression?
You might say, “Insurance is not paying for BOTOX for depression.”
I would say, “Whatever!?”
We are talking about a treatment that costs much less than a new set of tires. This is something that’s like buying a night in a hotel room every three months or, these days, filling your car with gas two or three times.
Not a Magic Bullet
First, just to repeat, I am at heart an internist; in no way do I think BOTOX is a magic bullet to cure everyone’s depression. All you know about the need for healthy living, treating addiction, the need for counseling, the need for good medical diagnosis–all of that and more still applies.
What I am saying is that (especially with the recent debunking of the serotonin “chemical imbalance” theory of depression), we do need more combination therapies and that BOTOX (because it is effective and safe) should be a commonly used tool to help those suffering the ravages of depression.
If you could be pregnant or if you have myasthenia gravis, you should not get BOTOX. Otherwise, I know of few therapies that have the potential for as much good with such a strong safety profile.
Thankfully, the same techniques that help people look better also help them feel better. So, when I do your BOTOX, I will be doing the very same thing I do when I treat frown lines (or the number 11’s).
My Request
If you think you would like to try BOTOX to help with your depression, DO NOT STOP TAKING ANY ANTIDEPRESSANTS YOU MAY BE TAKING; you can take your antidepressants and still use BOTOX to help them work better. Or, if you suffer a milder depression or anxiety (not on medications and not contemplating suicide) and want to see if BOTOX might help you feel better, then that is also good.
Here’s where to make an appointment with me<–
Best regards,

Charles Runels, MD
Savage Factors™ also helps with depression References
1.Argyriou AA, Mitsikostas DD, Mantovani E, Vikelis M, Tamburin S. Beyond chronic migraine: a systematic review and expert opinion on the off-label use of botulinum neurotoxin type-A in other primary headache disorders. Expert Review of Neurotherapeutics. 2021;21(8):923-944. doi:10.1080/14737175.2021.19586772.Caleo M, Restani L. Direct central nervous system effects of botulinum neurotoxin. Toxicon. 2018;147:68-72. doi:10.1016/j.toxicon.2017.10.0273.Zamanian A, Jolfaei AG, Mehran G. Efficacy of Botox versus Placebo for Treatment of Patients with Major Depression. :3.4.Mazzocchio R, Caleo M. More than at the Neuromuscular Synapse: Actions of Botulinum Neurotoxin A in the Central Nervous System. Neuroscientist. 2015;21(1):44-61. doi:10.1177/10738584145246335.Wise J. “No convincing evidence” that depression is caused by low serotonin levels, say study authors. BMJ. Published online July 19, 2022:o1808. doi:10.1136/bmj.o18086.Khademi M, Roohaninasab M, Goodarzi A, Seirafianpour F, Dodangeh M, Khademi A. The healing effects of facial BOTOX injection on symptoms of depression alongside its effects on beauty preservation. Journal of Cosmetic Dermatology. 2021;20(5):1411-1415. doi:10.1111/jocd.139907.Moncrieff J, Cooper RE, Stockmann T, Amendola S, Hengartner MP, Horowitz MA. The serotonin theory of depression: a systematic umbrella review of the evidence. Mol Psychiatry. Published online July 20, 2022. doi:10.1038/s41380-022-01661-08.Wollmer MA, Magid M, Kruger THC, Finzi E. The Use of Botulinum Toxin for Treatment of Depression. In: Whitcup SM, Hallett M, eds. Botulinum Toxin Therapy. Vol 263. Handbook of Experimental Pharmacology. Springer International Publishing; 2019:265-278. doi:10.1007/164_2019_2729.Al Abdulmohsen T, Kruger THC. The contribution of muscular and auditory pathologies to the symptomatology of autism. Medical Hypotheses. 2011;77(6):1038-1047. doi:10.1016/j.mehy.2011.08.044 -

United Airlines Drama
Here are 34 Reasons (and counting) why I fly Delta–not United
About 10 years ago, after noticing quite a bit of drama every time I flew United, I started keeping a few notes. I’m sure there are many amazing people who work for United. But, maybe the people they work for should pay more attention?
You can decide for yourself…
Baggage handler trapped in Cargo Hold during United flight
United Airlines: Fistfights, nude masturbation and dead pets: What’s going on with airline travel?
Passengers sue United Airlines after engine catches fire after takeoff: report
Dog dies in the luggage bin on United Flight
United Airlines flight diverted after man allegedly bites passenger’s ear, police say
United plane’s fan blade had multiple cracks; last inspected 4 years ago: NTSB. United Airlines
United Airlines emergency landing
United Airlines – New Jersey brothers kicked off flight for wearing scuba-like mask
EMT who treated dying United Airlines passenger finally notified of COVID-19 exposure 10 days later
Tomi Lahren scolds United for booting family with 2-year-old over toddler’s mask refusal: ‘Enough of this’
United Airlines agent stopped me for my ‘revealing’ shirt: Passenger
Disgusting’ passenger shamed for shaving his head during flight united airlines
Amsterdam-bound flight makes emergency landing in Maine. United Airlines
united airlines Airplane engine violently shakes midflight in terrifying footage
Couple claims United Airlines unfairly kicked them off flight: ‘We were traumatized’
United Airlines pilots arrested, accused of intoxication prior to US-bound flight from UK
CNN: united airlines Newark airport traffic delayed as plane makes unscheduled landing
United Airlines covers controversial seatback cameras
‘Rude’ United Airlines passenger slammed after complaining about middle sea
United Airlines passengers stranded on plane for over 14 hours at freezing airport in Canada
Former NBA star sues United Airlines over in-flight ‘race baiting’
United Airlines pilot cited for indecent exposure at Denver hotel: report. United Airlines
Plane goes partly off taxiway at Denver airport; no injuries. United Airlines
United Airlines angry passenger delays flight…
United Airlines. Mother worried because daughter denied her medicine
United Airlines Smoke causes need for emergency landing…
United Airlines sued by Nigerian passenger booted for ‘pungent’ odor, claiming racial discrimination